
Osteoporosis therapeutics have been proven to be effective in reducing the risk of vertebral and non-vertebral fractures. Ideally, they should be used as part of a multimodal therapy and tailored to individual patient characteristics. In view of the need for long-term treatment, particular attention must be paid to the management of rebound effects and side effects. Nowadays, it is suggested to take a break from therapy (“drug holidays”) after a few years.
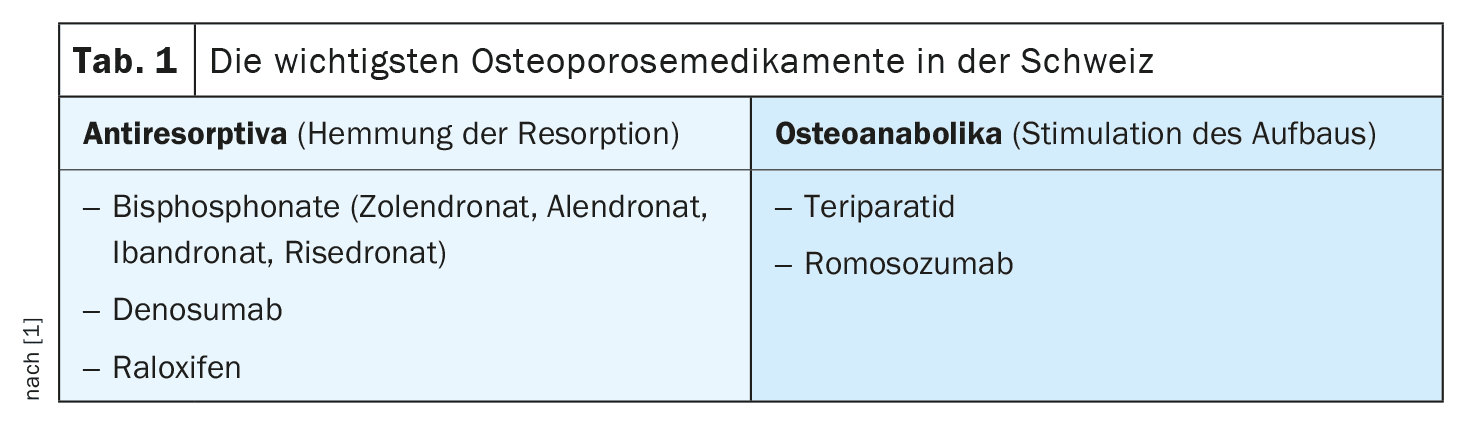
Dr. Adrian Forster, Head Physician, Schulthess Klinik, Zurich, and Dr. Regula Capaul, General Practitioner, Zurich-Oerlikon, gave a practical insight into the complex topic of osteoporosis therapy [1]. Today, around 20% of women and 7% of men over the age of 50 suffer from osteoporosis [2]. In Switzerland, this currently amounts to over 400,000 people affected. Osteoporosis is characterized by impaired remodelling of the bone substance and the resulting pathological microarchitecture of the bones. The reduced bone density leads to an increased risk of fractures. Older people and postmenopausal women are particularly affected by bone loss. Oestrogen deficiency, underweight and lack of exercise promote the development of osteoporosis. There are also a number of other risk factors. The most important groups of drugs for the treatment of osteoporosis in Switzerland are antiresorptives (bisphosphonates, denosumab, raloxifene) and osteoanabolic agents (teriparatide, romosozumab) (Table 1) [1]. All of these osteoporosis drugs can reduce bone mass loss and fracture risk, albeit to varying degrees [3].
Selection of an individually suitable bisphosphonate
Treatment with bisphosphonates has a proven benefit for long-term therapy of 3 to 5 years [3]. Zolendronate is currently the most potent substance with the highest bone affinity, according to Dr. Forster [1]. There is evidence of positive effects for this substance with regard to vertebral and non-vertebral fracture risk reduction [3]. However, side effects in the form of flu-like discomfort are relatively common in the first few days after a zolendronate injection, the speaker reported [1]. However, these usually disappear within a few days. One strategy to reduce the risk of side effects is to infuse the zolendronate rather slowly. For some patients, they would allow a whole hour for this. In addition, a non-steroidal anti-inflammatory drug or a painkiller based on paracetamol can be given beforehand, Dr. Forster advised [1]. Patients should also be sufficiently hydrated before a zolendronate infusion, as bisphosphonates are largely excreted via the kidneys. The speaker recommended using zolendronate only in patients with an eGFR >35 ml/min/1.73m2.
As an alternative to zolendronate, alendronate can be considered, as in the case study (box) . Ibronate is used with caution, as it has a lower bone affinity than zolendronate and alendronate and there are only data on the reduction of vertebral fracture risk, not peripheral fracture risk, according to the speaker [1].
Dr. Forster [1] also mentioned: “You should always correct a vitamin D deficiency before giving a bisphosphonate”. This is so that the bone can be adequately remineralized [1]. Vitamin D is known to support the storage of calcium in the bones; vitamin D supplementation is simple and inexpensive to implement.
| Case study: Fragility fracture of the thoracic spine |
| Dr. Capaul reported on the case of a 56-year-old female patient who fell at work on a slippery floor and sustained a fracture of the 12th thoracic vertebra (compression fracture). The orthopaedic surgeon prescribed conservative treatment with a 3-point corset, physical rest, concomitant analgesic therapy and radiographic follow-up. The patient was referred to the consultant for an osteoporosis assessment by her GP. The family history revealed that the patient’s sister had osteoporosis. The DEXA measurement showed osteoporosis in the lumbar spine and otherwise osteopenia. The consultant decided to initiate bisphosphonate therapy. At the time of the first zolendronate infusion, three months had passed since the fall. In the follow-up consultation with her GP six months later, the patient stated that she did not want another Zolendronate infusion due to the side effects in the days following the infusion (sleep disturbances, feeling of tension in the head). In consultation with a rheumatology specialist, the consultant decided to switch to alendronate (tablet, once a week) as an alternative, as this also had good data on the prevention of vertebral fractures. Alendronate proved to be well tolerated in this patient and a DEXA measurement after 2 years showed that there was no longer any osteoporosis in the lumbar spine. |
| according to [1] |
Essential measures after discontinuation of denosumab
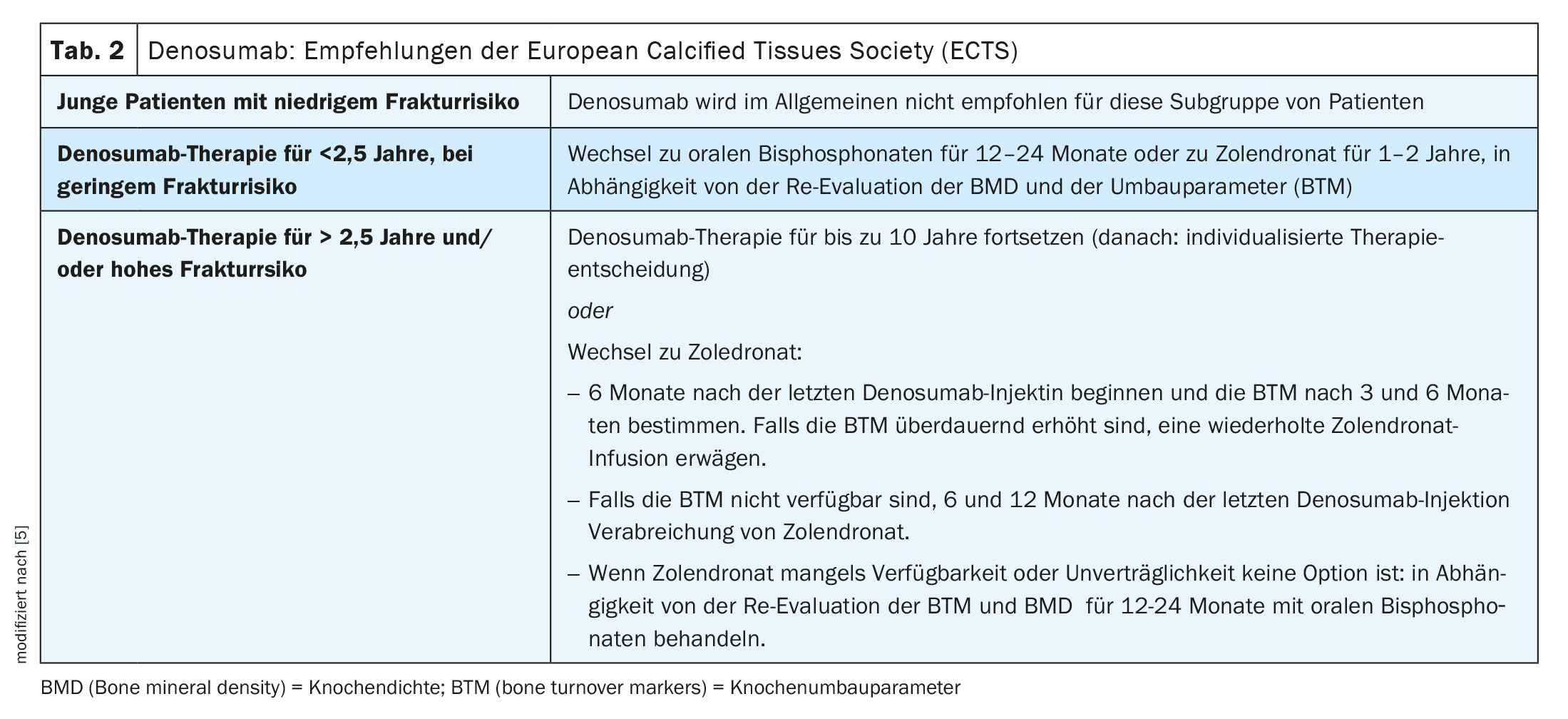
Denosumab has a proven benefit for up to 3 years [3]. Stopping treatment with denosumab leads to a complete and rapid reversal of the bone-specific effects. Therefore, other measures to maintain bone density must be used temporarily after discontinuation (Table 2). It was not until around 2016 that it was realized that a bisphosphonate must be given after discontinuation of denosumab, according to Dr. Forster [1]. Zolendronate is best suited, which is simply given at the time of the due denosumab injection. It is then worth measuring the remodeling parameters after 3 and 6 months in a fasting state. If these rise to the top third of the premenopausal norm, a second infusion should be given straight away. “Only when you see that the remodeling parameters remain low are you on safe ground,” explained the speaker [1]. Only then can a break in therapy be considered. If the remodeling parameters are not determined, zolendronate can simply be given 6 and 12 months after the last denosumab injection [1,5]. “Two infusions are needed,” emphasized Dr. Forster [1]. It used to be thought that a single infusion was sufficient. There are even patients in whom three infusions are necessary to adequately suppress the remodeling parameters. If zolendronate is not desired or not tolerated, alendronate can be used as an alternative. If treatment with denosumab is discontinued without subsequently administering a bisphosphonate, patients lose practically everything they have gained in the spine within 12 months, according to Dr. Forster [1].
Are jaw necrosis and atypical fractures preventable?
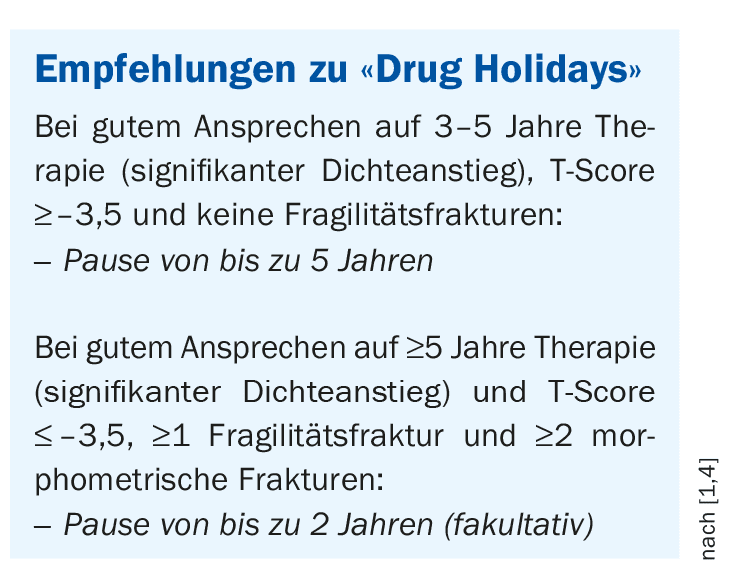
“Jaw necrosis and atypical fractures can be avoided, but it is relatively time-consuming,” Dr. Forster admitted [1]. In the case of mild osteoporosis, the speaker recommended taking a break from treatment for up to 5 years after a treatment period of 3-5 years. In the case of severe osteoporosis (low T-score, fragility fracture or morphometric vertebral fractures), a shorter break of up to 2 years could be considered. It is important to monitor patients during the treatment interruption, i.e. to take bone density measurements at regular intervals and to monitor bone remodeling in the laboratory. Depending on the results, the treatment break can be continued or a return to treatment can be considered (box). Regular dental check-ups are an important measure for patients with osteonecrosis of the jaw.
Congress: KHM Congress Lucerne
Literature:
- “Osteoporosis”, Seminar A1, Dr. med. Adrian Forster and Dr. med. Regula Capaul, KHM Congress Lucerne, 20.06.2024.
- Rheumaliga Schweiz: Osteoporose, brochure, 14th edition, 2022, www.rheumaliga.ch,(last accessed 04.07.2024).
- Obermayer-Pietsch B, Fössl I, Dimai HP: Long-term therapy concepts for osteoporosis [Long-term treatment concepts for osteoporosis]. Internist (Berl) 2021; 62(5): 474-485.
- McClung M, et al: Bisphosphonate therapy for osteoporosis: benefits, risks, and drug holiday. Am J Med 2013; 126(1): 13-20.
- Tsourdi E, et al: Fracture risk and management of discontinuation of denosumab therapy: a systematic review and position statement by ECTS. J Clin Endocrinol Metab 2020 Oct 26: dgaa756.
HAUSARZT PRAXIS 2024; 19(8): 44-45 (published on 23.8.24, ahead of print)









