In nonvalvular atrial fibrillation, treatment with oral anticoagulants is indicated. Many guidelines recommend the use of direct oral anticoagulants (DOAK) as first-line therapy. The advantage here is considered to be the elimination of regular INR monitoring and the ease of setting management. But is “one-dose-fits-all” really preferable?
Vitamin K antagonists (VKA) have been available for the prophylaxis of thromboembolic complications for about 50 years. They are used for oral anticoagulation for an artificial heart valve, atrial fibrillation or thrombophilia. With the introduction of DOAKs, the therapeutic options for anticoagulation have been expanded. This is also reflected in the frequency of prescriptions, which has increased significantly in recent years, especially for thrombin and factor Xa antagonists, as Prof. Heiner K. Berthold, MD, Bielefeld, Germany, explained. This development is also reflected in the guidelines, which predominantly recommend the preferred use of DOAKs. Not so, however, the Drug Commission of the German Medical Association (AkdÄ). It argues for preferential use of VKAs.
“There are definitely many advantages to using VKAs,” the expert said. This includes, for example, complete transparency about the potency and all influencing factors, as these are reflected in the INR. Through regular measurement, comedications, nutrition or even liver and kidney function can be monitored. Adherence can also be well monitored via INR measurement. “Once patients are well adjusted, they are easy to manage for years,” Berthold affirmed. This is sometimes due to the complexity of the active ingredients occurring at different times. While VKAs usually require intensive monitoring during the first four weeks of discontinuation, the complexity of DOAKs emerges over time. This may have implications for the kidneys, comedication, and in interventions. By closely monitoring INR during VKA therapy, the degree of anticoagulation can be monitored and a rapid response can be made if necessary.
Real-life data show superiority
Recent study results now also demonstrate significant superiority of VKAs over DOAKs [1]. The aim was to compare real-world data on efficacy and safety of the two therapeutic approaches in patients with atrial fibrillation. For this purpose, insurance data were analyzed from 11.1 million patients who had AF and whose diagnosis was confirmed by at least two outpatient diagnoses and/or a clinical diagnosis. They had received at least one outpatient prescription for a DOAK or VKA and had a CHA2DS2VAScscore >1 in the year before the initial prescription.
Two equally sized cohorts of 37,439 patients each with equivalent risk profiles were included in the analysis. The mean age was 78 years and the mean follow-up period was 12 months. It was shown that in almost every outcome parameter significantly more events occurred under DOAK therapy than under VKA (Fig. 1). Only hemorrhagic stroke was comparable in both groups.
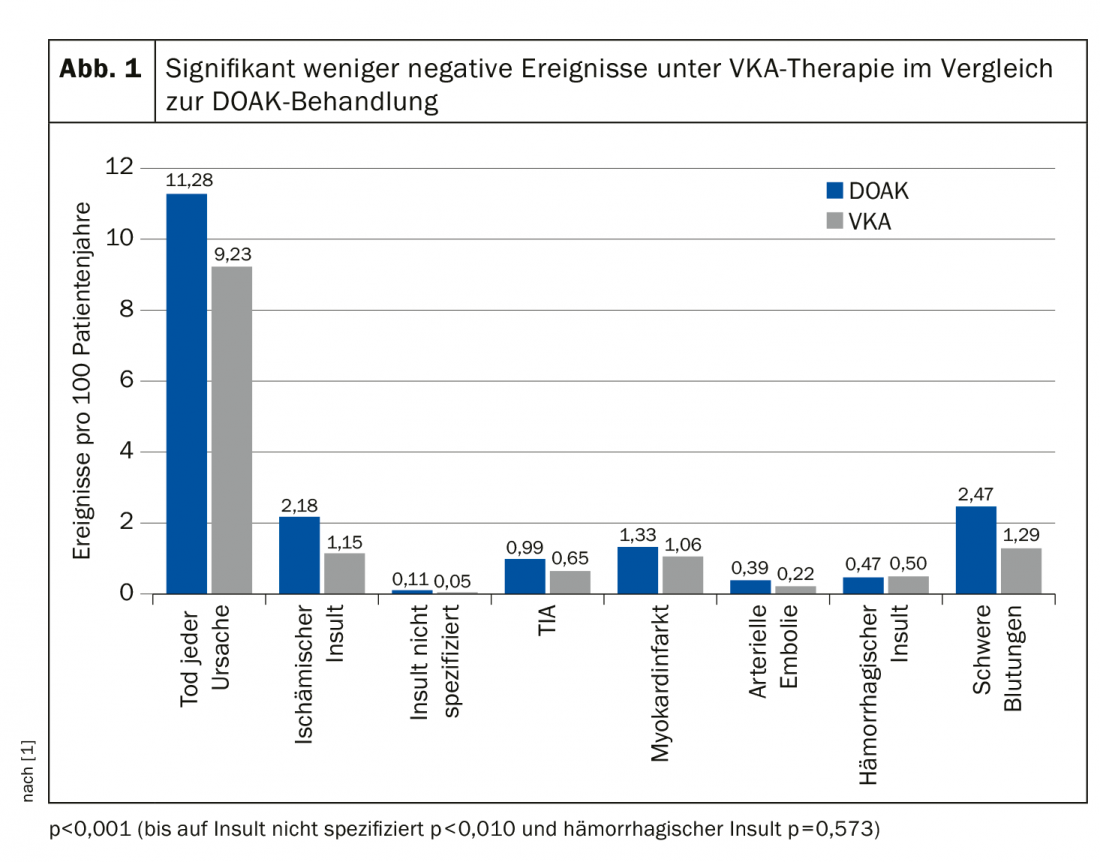
The quality of adjustment with VKA therapy seems to be very good, whereas that of DOAK administration is seen more critically by the authors. This is because about half of all patients received only low-dose therapy, even though there was often no diagnosis of renal insufficiency or failure. Accordingly, the optimum dosage was not achieved. In everyday practice, therefore, VKA therapy appears to be the more effective and safer choice.
Source: DGIM 2019, Wiesbaden (D)
Literature:
- Müller S, et al: Real-world effectiveness and safety of oral anticoagulation strategies in atrial fibrillation: a cohort study based on a German claims dataset. Pragmatic and Observational Research 2018; 9: 1-10.
HAUSARZT PRAXIS 2019; 14(9): 26 (published 9/30/19, ahead of print).