
The cardiology seminar at Medidays focused on three topics: blood pressure control, myocardial disease, and triple therapy for atrial fibrillation (AF) and stenting. In the treatment of resistant hypertension, renal sympathetic denervation has proven to be effective and safe, according to Prof. Thomas F. Lüscher, MD. Christiane Gruner, MD, went into more detail about the diagnostic pathways in hypertrophic cardiomyopathy. Finally, Jan Steffel, MD, referred to the potential of dual rather than triple therapy in VCF.
Prof. Dr. med. Thomas F. Lüscher, Clinic Director of Cardiology at the University Hospital Zurich, spoke in his lecture about hypertension treatment and pointed out that, in addition to increasing age, blood pressure is an important risk factor for stroke. Lowering blood pressure is associated with a reduced incidence of such events: “The incidence of cerebral strokes can be reduced by about 50%, and that of heart attacks by about 25%,” says Prof. Lüscher. This is not the only reason why arterial hypertension is a serious health problem worldwide, since, despite a variety of possible lifestyle interventions and pharmacological approaches internationally, the control of blood pressure is not satisfactory.
Renal sympathetic denervation
“The kidneys play a central role in long-term blood pressure regulation through efferent and afferent nerve fibers. It was discovered early on that surgical and pharmacological blockade of renal nerves can lead to reduced blood pressure. However, such an approach was also associated with an increase in noticeable side effects,” said Prof. Lüscher.
Catheter-based renal denervation represents a new therapeutic option to decrease the increased renal sympathetic nerve activity and tissue levels of norepinephrine (Table 1).
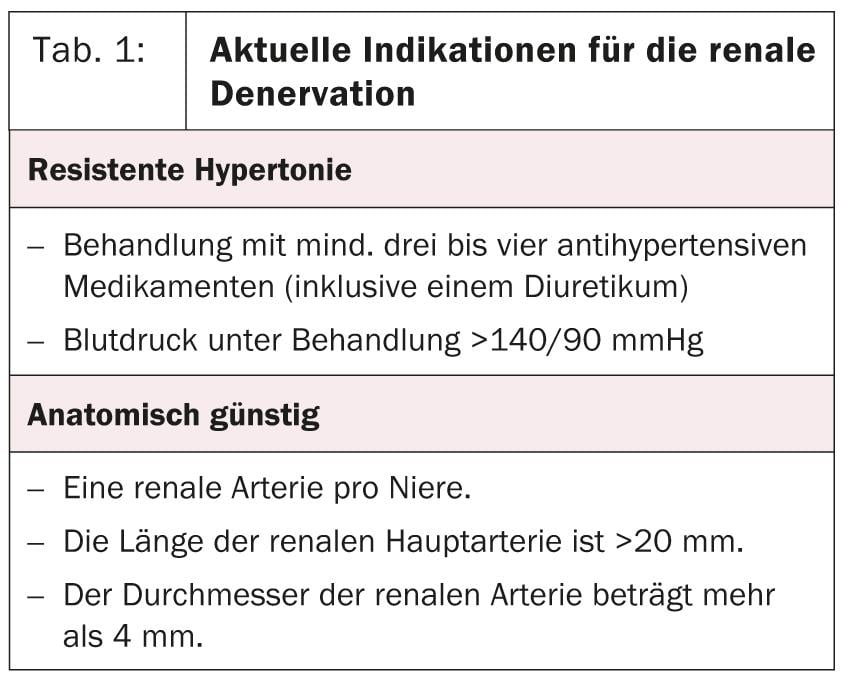
This was shown to be a safe and very effective strategy to control blood pressure in patients with resistant hypertension. Specifically, renal nerve ablation decreases blood pressure by 30 mmHg. “The reduction is not associated with changes in renal function or orthostatic hypotension. In contrast, renal denervation leads to an improvement in glucose metabolism,” Prof. Lüscher explained.
It should be investigated whether this treatment is a therapeutic option also for patients without resistant hypertension. Furthermore, it seems to have potential in the therapy of other diseases characterized by increased sympathetic activation (Table 2).

Complications
In the Simplicity HTN1 study, one patient suffered a renal artery dissection, and another developed a pseudoaneurysm at the femoral approach. Symplicity HTN2 demonstrated the development of an underlying arteriosclerotic lesion in a patient undergoing renal denervation but did not require treatment. “So the procedure has minimal complication rates,” summarizes Prof. Lüscher.
Cardiomyopathy
Dr. Christiane Gruner, MD, of the University Hospital Zurich, addressed the procedure and follow-up of myocardial diseases. Hypertrophic cardiomyopathy (HCM) is the most common inherited cardiomyopathy. It is defined by left ventricular hypertrophy (LVH) without dilatation and excluding other causes of LVH. Clinically, it usually presents at diagnosis as chest pain, shortness of breath, palpitations, cerebral apoplexy, syncope, or as a pathologic ECG. Family screening by ECG and echocardiography is useful in any case.
A reliable diagnosis can only be made by a multimodal approach using the following components: Anamnesis (individual/family), echocardiography, ECG and cardiovascular magnetic resonance imaging.
“Cardiac follow-up (ECG, echocardiography, Holter ECG, exercise stress test) should be performed once a year, and a cardiac MRI should be performed every three to five years to ensure optimal follow-up,” Dr. Gruner said.
In HCM, VHF is an associated problem in about 20% of cases. In this case, oral anticoagulation must be given in addition to beta-blockers, calcium antagonists, or amiodarone.
Triple therapy for atrial fibrillation
PD Dr. med. Jan Steffel from the University Hospital Zurich pointed out the problems regarding triple therapy (vitamin K antagonists, [VKA] + Aspirin® + clopidogrel/prasugrel/ticagrelor) in VCF and stenting: There are almost no data from randomized clinical trials; furthermore, the variety of clinical scenarios and patient-specific constellations (compliance, genetic variations, etc.) is large.
“In addition, triple therapy increases the risk of severe bleeding enormously: the so-called WOEST study investigated the occurrence of such bleeding as a primary endpoint and came to the conclusion that this can be significantly reduced by using a two-drug combination instead of a three-drug combination, i.e. by omitting Aspirin®. Whether the efficacy in preventing thrombotic events remains the same is not yet confirmed, as this secondary endpoint would need to be substantiated with further data. However, new evidence suggests that dual therapy is safe and effective, and the findings of the WOEST study point in this direction,” Dr. Steffel concluded.
Source: “Cardiology Update”, Seminar at Medidays, September 2-6, 2013, Zurich.
CARDIOVASC 2013; 12(6): 30-31









