
The treatment of bronchial carcinoma is greatly changed by immunotherapy. Current developments will lead to an adjustment of our therapy algorithms in the coming months.
The immune system can be thought of as a scale, with stimulating mechanisms on one side and blocking mechanisms on the other, finely tuned to provide protection against pathogenic structures (viruses, bacteria, and foreign substances) while preventing autoimmunity. Since the 2000s, more and more of these mechanisms have been identified on both sides of the scale. In particular, molecules from the group of so-called “immune regulatory checkpoints” appear to play a major role in the balance of the immune system. Antibodies that enable the activation of the immune system by blocking inhibitory immune regulatory checkpoint molecules are currently causing a sensation. These antibodies are available, for example, in the treatment of metastatic lung cancer and have become an integral part of the therapeutic repertoire. Their application is based on the premise that the tumor can be recognized by the immune system and that this immune response is at least partially blocked by the “immune regulatory checkpoints” PD-1/PDL-1.
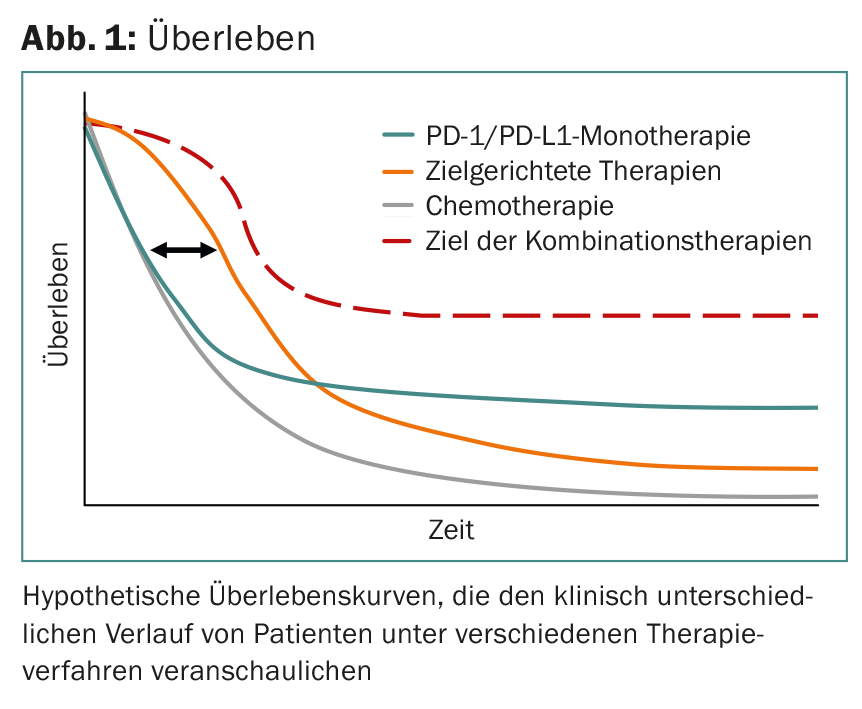
Based on the available data, this pathophysiologic scenario can be estimated to be present in 15-25% of all patients (in these patients, longer-term control of metastatic disease is established). This is taken as an indirect indication of control by the immune system and, conversely, also means that in approx. 80% of patients further immunosuppressive mechanisms are active or the immune system does not recognize these tumors in principle and thus no immune response can be “deblocked” (Fig. 1).
At the moment, there are no satisfactory assays that predict response to PD-1/PD-L1 blockade.
Metastatic lung cancer
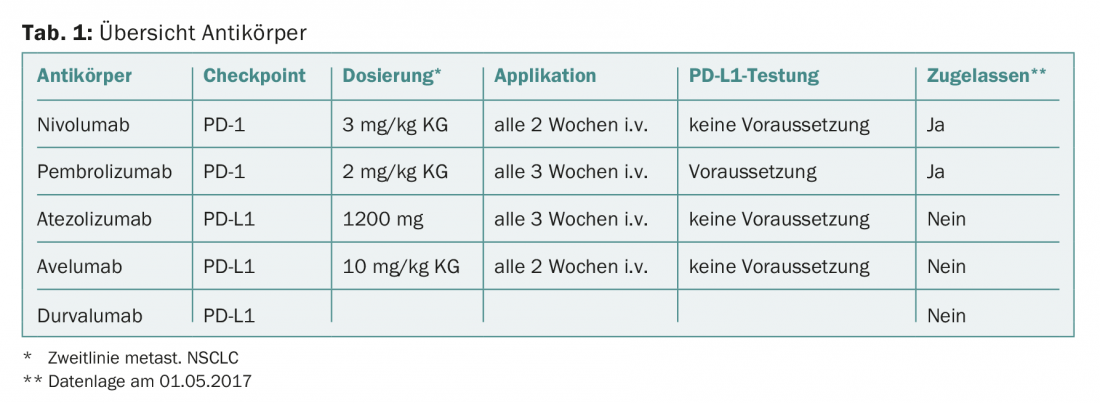
Antibodies are already approved in metastatic lung cancer (Table 1) that can prevent the activation of the PD-1/PDL-1 checkpoints and thus free the T cells from blocking the malignant tumor. Monoclonal antibodies can be divided into two groups: directed against PD-1 or directed against PD-L1.
First, nivolumab (anti-PD-1) received second-line approval in metastatic bronchial carcinoma independent of PD-L1 expression (Checkmate 057 and Checkmate 017). Compared with chemotherapy with docetaxel, 2-year overall survival improved by approximately 15% (median overall survival, “non-squamous”: 9.5 vs. 12.2 months; “squamous”: 6.0 vs. 9.2 months). The Checkmate 057 trial also demonstrated that in the absence of PD-L1 expression, improved 2-year overall survival can still be achieved compared with docetaxel (<1% of tumor cells: 25% vs. 18%). Therefore, approval was granted regardless of PD-L1 expression status. This clearly demonstrates the limitations of PD-L1 expression as a biomarker in bronchial carcinoma, as patients without PD-L1 expression in the tumor also derive clinical benefit from second-line therapy with nivolumab.
The development of pembrolizumab (anti-PD-1) is based on the assumption that, although PD-L1 is not a perfect biomarker, PD-L1 expression in tumor tissue is biologically important enough that its determination is necessary to justify checkpoint inhibition. Thus, only patients in whom PD-L1 expression could be detected (>1% of tumor cells) were included in the pivotal trials. The Keynote 010 trial showed a significant survival benefit compared with chemotherapy with docetaxel (median overall survival, “non-squamous”: 8.5 vs. 10.4 months).
Study results of nivolumab and pembrolizumab demonstrate that as PD-L1 expression increases, overall survival is improved when checkpoint inhibition (monotherapy) with an anti-PD-1 antibody is used. Both monoclonal antibodies thus highlight the important biological role of the PD-1/PDL-1 checkpoint, but based on the results do not allow it to be used as the sole biomarker, as patients without PD-L1 expression in the tumor also benefit.
Atezolizumab, durvalumab, and avelumab target PD-L1 and theoretically have a slightly different immunologic profile. Anti-PD-L1 antibodies only block the interaction between PD-L1 and PD-1 and not between PD-L1/-L2 and PD-1 as an anti-PD-1 antibody does. This difference could lead to a more favorable side effect profile. In addition, more stimulatory receptors are theoretically available for T cells to use through the interaction of B7.1 and PD-L1. However, since no comparative studies between anti-PD-1 and anti-PD-L1 antibodies have been performed so far, the postulated clinical advantage in terms of better efficacy and fewer undesirable side effects is not proven. Atezolizumab demonstrated a significant survival benefit compared to docetaxel in a phase III study (OAK study) (median overall survival, “non-squamous”: 11.2 vs. 15.6 months; “squamous”: 7.7 vs. 8.9 months). Data from a phase II study (ATLANTIC study) are available for durvalumab as monotherapy. This study consists of three cohorts for patients after failure of second-line therapy, whose overall survival was analyzed according to PD-L1 expression level (median overall survival, <25% of tumor cells: 9.3 months; >25% of tumor cells: 10.9 months; >90% of tumor cells: not reached at 12 months). Avelumab demonstrated an “overall response rate” of 11.6 weeks for PD-L1-positive (>25% of tumor cells) and 6.0 weeks for PD-L1-negative (<25% of tumor cells) tumors in a phase IB trial (JAVELIN Solid Tumor) in second-line therapy.
All PD-1/PD-L1 checkpoint inhibitors have a similar side effect profile. Grade 3-4 adverse events occurred in 2-5% of all patients across all studies and included pneumonitis, elevated transaminases, and thyroid dysfunction.
Summary
In the end, treating oncologists will be spoiled for choice, as multiple checkpoint inhibitors are rapidly becoming available starting in second-line metastatic bronchial carcinoma. All antibodies show a similar spectrum of activity or side effects. Primarily, the antibodies differ clinically in terms of dosage and frequency of application (Table 1).
The use of PD-1/PD-L1 checkpoint inhibitors will also change significantly again in the coming weeks, as pembrolizumab is now also approved in Switzerland in the first line for bronchial carcinomas expressing >50% PD-L1. Thus, in the second line, chemotherapy should regain a more important role and PD-L1 testing should become a key diagnostic prior to first-line therapy with great therapeutic relevance.
Furthermore, it can be assumed that combination therapies can be used in the foreseeable future – either as checkpoint inhibition with chemotherapy or two checkpoint inhibitors in combination. Thus, second-line PD-1/PD-L1 blockade monotherapy will also become less important in metastatic bronchial carcinoma.
Take-Home Messages
- The treatment of bronchial carcinoma without a detectable Driver mutation is undergoing major changes at the moment due to immunotherapy.
- Current developments will lead to an adjustment of our therapy algorithms in the coming months.
InFo ONCOLOGY & HEMATOLOGY 2017; 5(3): 14-16.









