
At the swissESCupdate, cardiology experts summarized important content from this year’s Annual Meeting of the European Society of Cardiology . In the area of heart failure, studies on the use of mineralocorticoid receptor antagonists (MRAs) were a dominant topic. The bottom line is that the current study situation reinforces the importance of MRAs in heart failure therapy.
It has long been empirically proven that MRAs contribute to a reduction in morbidity and mortality in patients with HFrEF. The FINEARTS-HF study was conducted to assess the efficacy and safety of finerenone – a non-steroidal MRA – in patients with HFmrEF and HFpEF, reported Prof. Dr. med. Felix Mahfoud, Head of Cardiology and Professor of Cardiology at the Faculty of Medicine of the University of Basel [1,2]. In this double-blind international study, patients with heart failure and an LVEF ≥40% were randomized in a 1:1 ratio to finerenone (at a maximum dose of 20 mg or 40 mg once daily) or a corresponding placebo, in each case in addition to standard treatment. The primary endpoint was a composite of events** leading to worsening heart failure and death from cardiovascular causes. The total number of events leading to worsening heart failure was 842 in the finerenone group and 1024 in the placebo group (relative risk 0.82; 95% CI, 0.71-0.94; p=0.006). The percentage of patients who died from cardiovascular causes was 8.1% and 8.7%, respectively (hazard ratio [HR] 0.93; 95% CI, 0.78-1.11). Finerenone was associated with an increased risk of hyperkalemia and a decreased risk of hypokalemia.
** event was defined as: first or repeated unplanned hospitalization or emergency consultation due to heart failure
| Abbreviations |
| HFrEF = heart failure with reduced ejection fraction |
| HFmrEF = heart failure with slightly reduced ejection fraction |
| HFpEF = heart failure with preserved ejection fraction |
| LVEF = left ventricular ejection fraction |
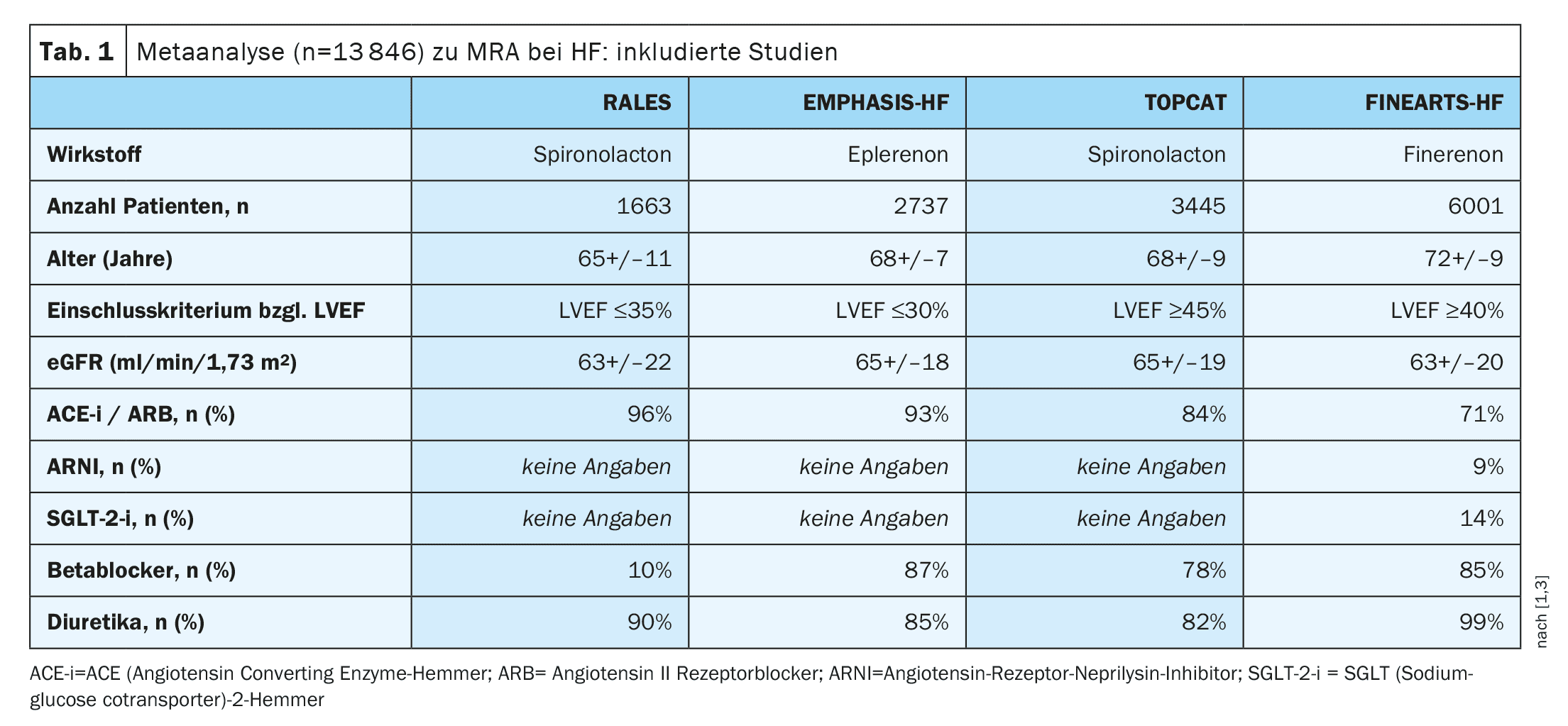
Meta-analysis based on four large clinical studies
Prof. Mahfoud also presented the results of a meta-analysis, which encourage the use of MRA across the entire spectrum of ejection fraction [1,3]. A total of 13,846 patients from the following studies were included in the analyses:
- FINEARTS-HF for Finerenon
- RALES and TOPCAT for spironolactone
- EMPHASIS-HF for eplerenone
The average age of the study participants was between 65 and 72 years (Table 1). The overall results showed that a significant reduction in heart failure-related hospitalizations was observed in both the HFrEF trials and the HFmrEF or HFpEF trials (HR 0.63; 95% CI: 0.55-0.72 and HR 0.82; 95% CI 0.74-0.91, respectively) [3]. Due to the greater efficacy in HFrEF compared to HFmrEF or HFpEF, there was a statistically significant interaction by study and treatment (p for interaction=0.0012). Cardiovascular mortality was significantly reduced only in the HFrEF trials, but not in the HFmrEF or HFpEF trials (HR 0.72; 95% CI: 0.63-0.82 and HR 0.92; 95% CI: 0.80-1.05, respectively). The same pattern was seen for the risk of dying from any cause (HR 0.73; 0.65-0.83 and HR 0.94; 0.85-1.03, respectively). Despite the interaction between the study types, sensitivity analyses confirmed the robustness of the results. The risk of hyperkalemia is known to be increased with MRA. In the meta-analysis, the odds ratio [OR] compared to placebo was 2.27 (95% CI 2.02-2.56).
However, the incidence of severe hyperkalemia$ was low (2.9% vs. 1.4%) and the risk of hypokalemia& was only half that of placebo (OR 0.51; 0.45-0.57). With regard to episodes of low systolic blood pressure, the MRA study arm and placebo arm differed only slightly.
$ Serum potassium >6.0 mmol/l
& potassium <3-5 mmol/l
Overall, the present meta-analysis indicates that steroidal MRAs in patients with HFrEF and non-steroidal MRAs in patients with HFmrEF or HFpEF have been shown to have clinically relevant benefits, the speaker explained [1]. As the protective effects of MRA were consistent across different patient subgroups, the results suggest that MRA should be considered in heart failure patients without contraindications in the future.
Another study Prof. Mahfoud mentioned was the RESHAPE2 study (n=505), in which transcatheter mitral valve repair in addition to drug therapy resulted in a lower rate of first or recurrent heart failure-related hospitalizations and a reduction in cardiovascular mortality after 24 months in patients with heart failure and functional mitral regurgitation, compared to drug treatment alone [1,4].
Congress: swissESCupdate.24
Literature:
- “Heart Failure”, Prof. Dr. Felix Mahfoud, Hotline, Session 3, SwissESCUpdate, Basel, 05.09.2024.
- Solomon SD, et al; FINEARTS-HF Committees and Investigators. Finerenone in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med 2024 Oct 24; 391(16): 1475-1485.
- Jhund PS, et al: Mineralocorticoid receptor antagonists in heart failure: an individual patient level meta-analysis. Lancet 2024 Sep 21; 404(10458): 1119-1131.
- Anker SD, et al; RESHAPE-HF2 Investigators. Transcatheter Valve Repair in Heart Failure with Moderate to Severe Mitral Regurgitation. N Engl J Med 2024 Aug 31. doi: 10.1056/NEJMoa2314328.
HAUSARZT PRAXIS 2024; 19(11): 36–37 (published on 22.11.24, ahead of print)
CARDIOVASC 2024; 23(4): 35–36









